
In a study posted to the medRxiv* preprint server, researchers conducted a systematic review and meta-analysis to determine the household secondary infection attack rate (hSAR) of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).
SARS-CoV-2, which causes coronavirus disease 2019 (COVID-19), was initially reported in Wuhan, China, and declared a pandemic in March 2020 by the World Health Organization (WHO). Since the early pandemic, households have served as significant transmission pools for SARS-CoV-2. The first few X cases (FFX) in households and household transmission investigations (HHTIs) are essential for understanding the transmission dynamics of SARS-CoV-2 and COVID-19 severity.
The WHO developed a suite of standardized protocols in response to the emergence of novel SARS-CoV-2; these early studies were labeled as unity studies and included both FFX investigation and HHTI protocols.
 Study: Transmission of SARS-CoV-2 in standardised First Few X cases and household transmission investigations: a systematic review and meta-analysis. Image Credit: Lightspring / Shutterstock
Study: Transmission of SARS-CoV-2 in standardised First Few X cases and household transmission investigations: a systematic review and meta-analysis. Image Credit: Lightspring / Shutterstock
The study
In the current study, researchers systematically reviewed, meta-analyzed, and summarized the available FFX and HHTI data for SARS-CoV-2. The study’s primary outcome was hSAR estimation, defined as the probability of SARS-CoV-2 infection among those susceptible in the household upon exposure to the first confirmed COVID-19 case. The secondary outcome was to measure the household secondary clinical attack rate (hSCAR), defined as earlier but with clinical criteria alone.
Data for the systematic review were obtained from the following sources: MEDLINE, Web of Science, Scopus, and Embase, which were explored to retrieve relevant studies published between December 1, 2019, and July 26, 2021. The second source was preprint servers such as bioRxiv and medRxiv, wherein unpublished investigation data were available. Lastly, the team screened FFX and HHTI results unavailable in the literature but shared directly by the collaborators of unity studies with the WHO before October 1, 2021.
Studies were eligible if 1) aligned to the WHO unity studies’ FFX and HHTI protocols and had longitudinal data collection with active household follow-up, 2) included a minimum of five households, 3) reported hSAR/hSCAR or provided data to calculate them, 4) published in English, French, Chinese, Russian, Portuguese, Spanish, Italian or German, and 5) represented original investigations.
A critical appraisal tool was developed for methodological quality assessment that comprised 12 items assessing the specific aspects of the HHTI design. Five members independently evaluated the methodological quality. Subsequently, the investigations were categorized as having a low, moderate, or high risk of bias based on the methodological quality. The hSAR, hSCAR, and 95% confidence intervals (CIs) were meta-analyzed to estimate the global SARS-CoV-2 hSAR or hSCAR.
Findings
The research team initially identified 9,954 published records by searching the databases and 34 FFX and HHTIs from WHO unity studies collaborators. Upon screening, 80 investigations were finalized for data extraction, including 64 from databases and 16 from unity studies collaborators. Of these, 62 investigations (51 from databases and 11 from collaborators) were considered for the meta-analysis. The investigations included for hSAR estimation (primary outcome) provided descriptions for household follow-up between January 2020 and July 2021; two did not mention the start date. Overall, the investigations covered 32 countries across six WHO regions, with 15 countries contributing more than one investigation. Twenty articles for the (systematic) review were contributed from China, eight from India, seven from the United States, and four from South Korea and Canada. About 15 Lower- and middle-income countries (LMICs) contributed 41 (51%) investigations for the systematic review, of which 32 were meta-analyzed. High-income countries (HICs) contributed 39 investigations for the review, with 30 included in the meta-analysis. Around 43 studies were explicitly designed for HHTI.
Seventy-six investigations reported an hSAR in contrast to 33 investigations, which reported hSCAR. Of the 76 investigations, a low risk of bias was estimated for 25, moderate for 38, and high for 13 studies. Among the 33 hSCAR-reporting investigations, 22 were considered low risk of bias and 11 with moderate risk of bias.
Eighteen studies were excluded from the meta-analysis due to a high risk of bias, lack of hSAR, or inclusion of highly vaccinated cohorts. The hSAR point estimates ranged from 2% to 90%, and the 95% prediction intervals also varied (3% to 71%), indicating substantial heterogeneity among the investigations. Similar heterogeneity was evident with hSCAR studies, and hence pooled estimates of hSAR or hSCAR were not reported.
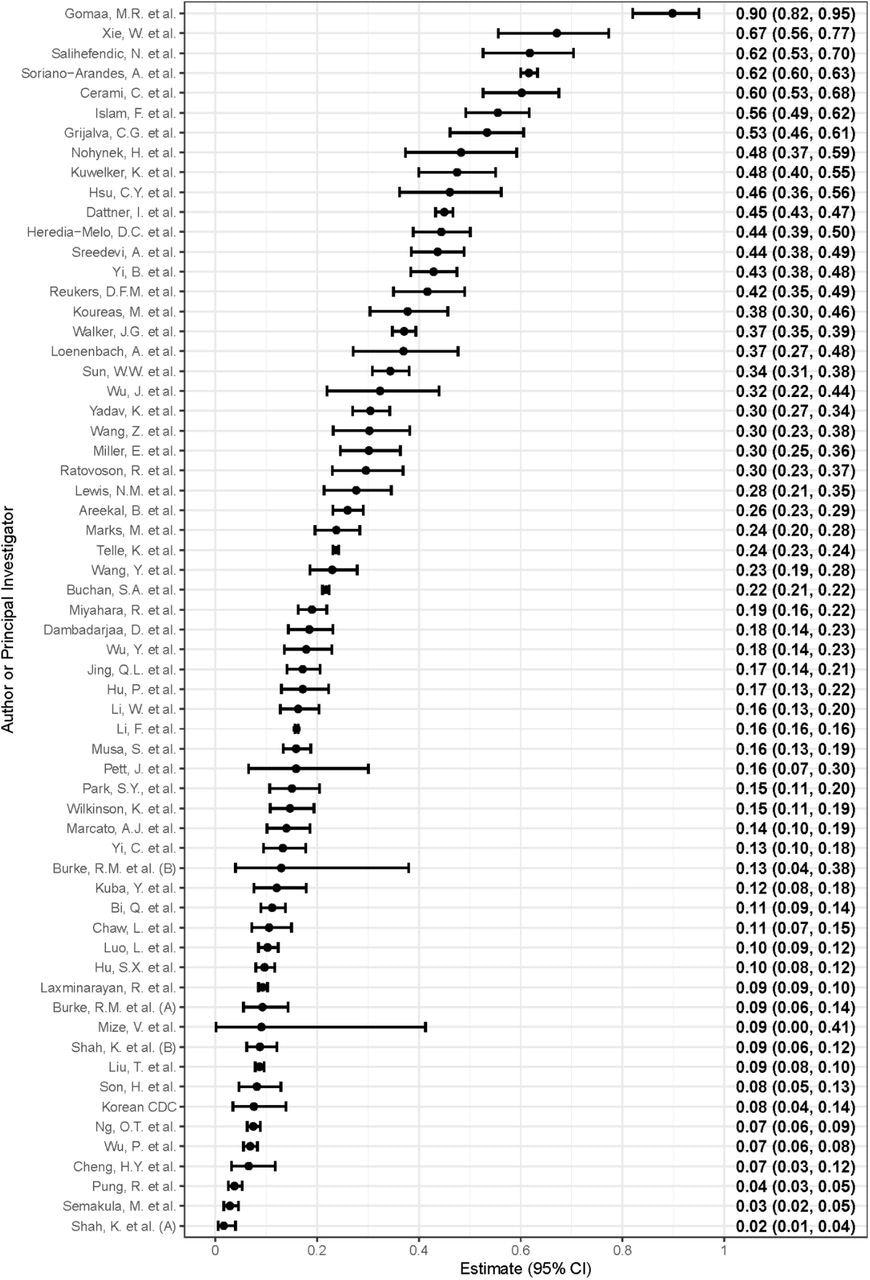
Forest plot of the household secondary infection attack rates (hSAR) in included investigations (n = 62), ordered from highest estimated hSAR (top) to lowest estimated hSAR (bottom). The hSAR and 95% confidence intervals (CI) are shown on the right margin.
Conclusions
According to the authors, the present study was the first to systematically review and meta-analyze standardized FFX, and HHTIs aligned with the WHO unity studies’ HHTI protocols for SARS-CoV-2. Over 51% of these were contributed from LMICs, indicating the feasibility of implementation across the WHO regions in different settings.
With the continued progression of the COVID-19 pandemic, FFX and HHTI studies are essential as critical tools for monitoring population immunity against transmission dynamics and severity of SARS-CoV-2. While the WHO unity studies framework is potent enough to guide HHTIs, the significant variance in hSAR estimates emphasizes the need to improve standardization in the planning, conduct, and analysis for comprehensive reporting of FFX and HHTIs.
*Important notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
Journal reference:
- Transmission of SARS-CoV-2 in standardised First Few X cases and household transmission investigations: a systematic review and meta-analysis. Hannah C Lewis, Adrian J Marcato, Niamh Meagher, Marta Valenciano, Juan-Pablo Villanueva-Cabezas, Violeta Spirkoska, James E Fielding, Amalia Karahalios, Lorenzo Subissi, Anthony Nardone, Brianna Cheng, Soatiana Rajatonirina, Joseph C Okeibunor, Eman A Aly, Amal Barakat, Wasiq Khan, Pernille Jorgensen, Tasnim Azim, Pushpa Ranjan Wijesinghe, Linh-Vi Le, Angel Rodriguez, Andrea Vicari, Maria Van Kerkhove, Jodie McVernon, Richard Pebody, David J Price, Isabel Bergeri, the Unity Studies Collaborator Group, medRxiv preprint 2022, DOI: https://doi.org/10.1101/2022.04.01.22273107, https://www.medrxiv.org/content/10.1101/2022.04.01.22273107v1