Despite high remission rates for patients treated with T cells that are supercharged in laboratories into elite cancer warriors, there is still a considerable population of patients who eventually relapse, their cancers invariably coming back.
It is estimated that CAR T cell therapy—a breakthrough form of cancer immunotherapy—has a 30 percent to 40 percent rate of success for durable remission. That means a significant number of patients aren’t quite as lucky. To improve the odds, medical scientists in laboratories worldwide are searching for ways to make CAR T cell cancer therapy work more effectively.
CAR T cells—chimeric antigen receptor T cells—start out as the patients’ own T cells isolated from a blood sample, but the cells are primed in a laboratory using a genetic modification process that causes T cells to express a cancer-seeking-and-destroying receptor on their surface.
That special receptor is known as the chimeric antigen receptor, or CAR, engineered to bind to a specific target— the cancer’s antigen—a molecular complex known as CD19. Cancer cell destruction can be swift—indeed, so much so that the therapy has been known to quickly force some cancers into remission. CAR T cell therapy is used in the treatment of certain cancers of the blood, primarily acute lymphoblastic leukemia, B-cell lymphoma, follicular lymphoma and multiple myeloma.
CAR T cells’ population is expanded into a formidable army before being transfused into the patient. A lab grows millions of altered T cells before shipping them back to the patient’s hospital. Once returned, the modified T cells are stronger, bolder and cancer-seeking. Bearing the chimeric antigen receptor allows these T cells to hunt down and destroy cancer cells. Because they seek and destroy malignant cells around the clock, some doctors have referred to CAR T cell therapy as “a living drug.”
“Immunotherapy with chimeric antigen receptor cells has emerged as a promising therapeutic tool against cancer,” asserted Dr. Afroditi Katsarou, reporting in Science Translational Medicine. Even though the therapy works best in hematological cancers, it is not recommended for all forms of these malignancies. The approach remains under study as a form of treatment for solid tumors, which don’t have as high a response rate to CAR T cells as cancers of the blood, although emerging clinical studies hint at eventual success.
Katsarou, lead author of the new research, along with a team of scientists in the department of hematology at Amsterdam University Medical Centers in the Netherlands, are embarking on a novel approach that involves attaching not one, but two engineered receptors to T cells. Scientists from throughout the Netherlands are working with the Amsterdam-based team, as well as with a collaborative group of international scientists, including American researchers at Memorial Sloan Kettering Cancer Center in New York and Harvard Medical School in Boston.
Their aim is solve one of the biggest problems in CAR T cell cancer therapy: It doesn’t work for everyone. Cancers rebound in what the scientists describe as a considerable proportion of patients. The Amsterdam-led team theorizes that a dual-receptor strategy can increase the effectiveness of this form of immunotherapy and lower the rate of treatment failures.
The scientists posit that T cells wielding two receptors can double the capability of CAR T cells to fight cancer. Using a dual strategy additionally enhances the persistence of CAR T cells in the blood. It is therefore hoped that this new breed of CAR T cells can track down stealthy malignant cells that elude traditional single-receptor CAR T cells. Having two receptors diminishes the possibility of cancer cells seeding a re-emergence, sending patients into a relapse, scientists say.
“Second-generation CARs that provide combined activation and co-stimulatory signals have been shown to induce impressive clinical responses,” Katsarou wrote in Science Translational Medicine.
Not long after the first CAR T cell therapies were first approved nearly five years ago, doctors noticed the therapy worked better for some patients with hematological cancers than others. “CARs are highly reliant on target antigen density, and, as a consequence, CAR T cells lose their functionality when antigen expression drops below a [certain] threshold,” Katsarou wrote.
Most relapses occur either because the CAR T cells don’t persist long enough after transfusion, according to the team of researchers, or because the CAR T cells struggle to recognize cancer cells that harbor fewer antigens to target. “T cell exhaustion and reduced persistence are other major factors limiting the efficacy of CAR T cells,” the collaborating group reported.
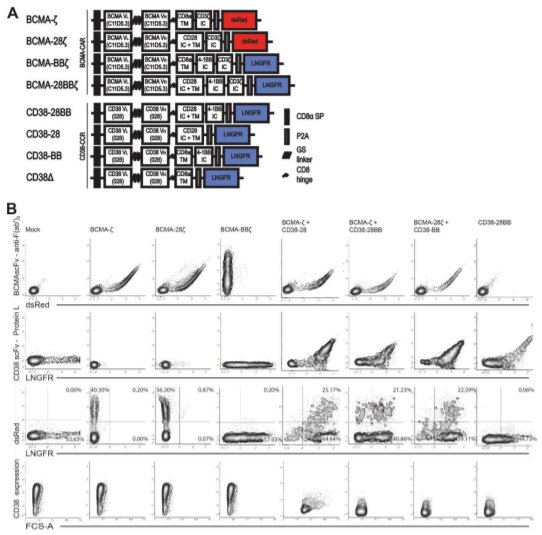
In their study, Katsarou and colleagues tested dual-receptor T cells in laboratory dishes and in an animal model. The cells’ performance suggests that this type of modification could address the twin challenges of poor CAR T cell longevity and ineffectiveness against low-antigen density, which prevent the altered cells from working for many patients. Key to the research were the two types of receptors introduced to T cells. One was the traditional chimeric antigen receptor and the other a chimeric costimulatory receptor, or CCR.
Compared with traditional CAR T cells, the CAR-CCR T cell combination was more sensitive “to low-antigen multiple myeloma and leukemia cells in culture,” the scientists reported in their research. The new dual receptor T cells also expanded and persisted longer in mouse models of multiple myeloma and low-antigen leukemia, which extended survival times and delayed cancer progression, the researchers found.
CAR T cell therapy, also known simply as CAR T, was pioneered by medical scientists Isabelle Rivière, Michel Sadelain and Renier Brentjens of Memorial Sloan Kettering Cancer Center in New York. Their deceptively simple hypothesis that T cells, if modified, could vanquish cancer became the basis for a series of laboratory and clinical studies, which took nearly 20 years. The first drugs capable of coaxing the expression of chimeric antigen receptors on T cells were approved in 2017.
This kind of therapy is defined as individualized—or customized—because patients’ own cells are the key ingredients. Doctors send patients’ blood samples to the drug manufacturer’s laboratory, where the T cells are modified to recognize the cancer target,OK CD19. It can take up to three weeks for the supercharged cells to return to patients’ hospitals.
Currently, there are five CAR T cell drugs that have been approved by the U.S. Food and Drug Administration: Abecma (idecabtagene vicleucel); Breyanzi (lisocabtagene maraleucel); Kymriah (tisaglenlecleucel); Tecartus (brexucabtagene autoleucel), and Yescarta (axicabtagene ciloleucel).
Side effects among patients transfused with the altered T cells have included fever, dizziness, lightheadedness, nausea, vomiting and diarrhea. More serious side effects also have been documented, such as irregular heartbeats and difficulty breathing.
Scientists hope the early research involving dual-receptor T cells lays the groundwork for a new way to deliver the therapy. “The application of this strategy could improve clinical outcomes and accelerate the progress of CAR T cell therapy for various malignancies,” Katsarou and the team concluded.
CAR-T immunotherapy could be improved to kill solid tumors
Afroditi Katsarou et al, Combining a CAR and a chimeric costimulatory receptor enhances T cell sensitivity to low antigen density and promotes persistence, Science Translational Medicine (2021). DOI: 10.1126/scitranslmed.abh1962
© 2022 Science X Network
Citation:
In the lab: T cells artificially endowed with 2 cancer-seeking receptors aim to be an elite army of cancer killers (2022, January 14)
retrieved 14 January 2022
from https://medicalxpress.com/news/2022-01-lab-cells-artificially-endowed-cancer-seeking.html
This document is subject to copyright. Apart from any fair dealing for the purpose of private study or research, no
part may be reproduced without the written permission. The content is provided for information purposes only.

{kind=link}